
GI Oncology & Cancer Surgery
Cancer of the digestive tract requires more than just surgery; it requires a strategy. Dr. Srinivas Bojanapu leads a specialized unit focused on the "Chemical Factories" of the body—the Stomach, Colon, Liver, and Pancreas. By combining Robotic Precision (Da Vinci Xi) with Multidisciplinary Tumor Boards, we aim for "R0 Resection" (complete removal) while preserving your ability to eat, digest, and live normally.
The Treatment Roadmap
We believe in transparency. Every patient follows a structured clinical pathway to ensure no step is missed, from the first scan to long-term survivorship.
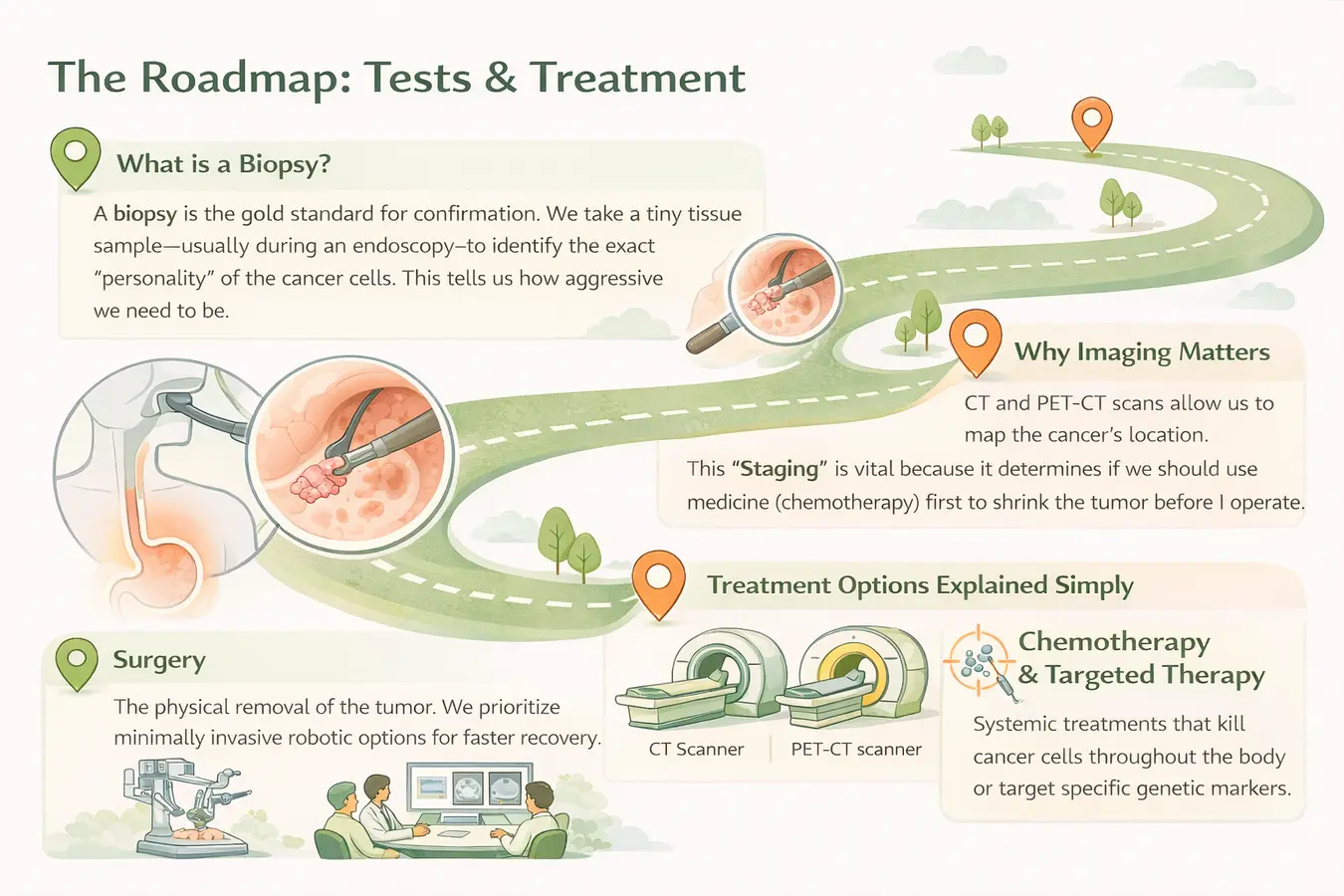
Phase 1: Accurate Staging (The Foundation)
Before we cut, we must see. We utilize PET-CT Scans and Endoscopic Ultrasound (EUS) to stage the cancer precisely. We don't just ask "Is there cancer?" we ask "Exactly which layer of the wall is it in?" This determines if we need chemotherapy before surgery (Neoadjuvant therapy).
Specialized Cancer Centers
The digestive system is complex. We have dedicated protocols for each organ.
Colon Cancer
Protocol: Robotic Colectomy with Complete Mesocolic Excision (CME). We remove the tumor and the entire lymphatic drainage basin to prevent recurrence.
Stomach Cancer
Protocol: D2 Radical Gastrectomy. This involves removing the stomach and specific lymph node stations (1-12) tailored for Gastric Adenocarcinoma.
Pancreatic Cancer
Protocol: The Whipple Procedure (Pancreaticoduodenectomy). A complex reconstruction of the bile duct, stomach, and intestine after removing the tumor.
Liver Cancer (HCC)
Protocol: Precision Hepatectomy using CUSA technology. For cirrhotic patients, we offer Liver Transplantation as a curative option.
Rectal Cancer
Protocol: Sphincter-Preserving Surgery (TME). We use robotics to work in the narrow pelvis, saving the natural passage and avoiding a permanent bag.
Esophageal Cancer
Protocol: Thoracoscopic McKeown’s Surgery. Minimally invasive removal of the food pipe for patients with difficulty swallowing (Dysphagia).
The Robotic Advantage (Da Vinci Xi)
It is not a gimmick; it is a necessity for precision. In the narrow spaces of the pelvis (Rectum) or the deep retroperitoneum (Pancreas), human hands are limited. The Da Vinci Xi Robot gives us:
- 3D High-Definition Vision: We see nerves and blood vessels magnified 10x, allowing us to spare them. This is crucial for preserving urinary and sexual function in rectal cancer surgery.
- 7 Degrees of Freedom: The instruments bend and rotate far beyond the capability of the human wrist, allowing us to suture in tight spaces.
- Tremor Filtration: The computer eliminates even microscopic hand tremors for perfect anastomosis (joining of tissues).
- Firefly Fluorescence: We inject a green dye (ICG) that makes the tumor blood supply "glow," ensuring we only cut where it is safe.
Symptom Checker: When to Worry?
GI cancers are often "Silent Killers" in early stages. However, subtle signs usually exist. Do not ignore these red flags.
| Organ | Early Warning Signs (Consult Us) | Advanced Signs (Urgent) |
|---|---|---|
| Stomach | Persistent acidity, feeling full after small meals. | Vomiting blood, black stools (Melena). |
| Colon/Rectum | Change in bowel habits (Constipation/Diarrhea). | Blood in stool, pencil-thin stools. |
| Pancreas | Vague back pain, sudden onset diabetes. | Painless Jaundice (Yellow eyes), weight loss. |
| Esophagus | Feeling food "sticking" in the chest. | Unable to swallow solids, weight loss. |
The Tumor Board & Genetics
Cancer care is never a one-man show. At our center, every single case is presented to a Multidisciplinary Tumor Board before we touch the patient.
Surgical Oncologist
Planning the operation.
Medical Oncologist
Planning Chemotherapy.
Radiation Oncologist
Targeting localized spread.
Pathologist
Decoding tumor biology.
Genetic Screening
For young patients or those with a strong family history, we conduct genetic testing (e.g., Lynch Syndrome, BRCA). If a genetic mutation is found, we may alter the surgical plan to be more extensive to prevent future cancers, and we screen your family members as well.
Enhanced Recovery (ERAS) & Nutrition
The old days of starving patients for 5 days after surgery are gone. We follow ERAS Protocols to get you home faster.
- Carbohydrate Loading: You drink a special energy drink 2 hours before surgery to reduce stress on the body.
- Opioid-Free Anesthesia: We use nerve blocks (Epidurals) to control pain without the side effects of strong painkillers like drowsiness or constipation.
- Early Feeding: Most patients drink liquids on Day 1 and eat soft food by Day 3. This prevents the gut from "going to sleep" (Ileus).
- Early Mobilization: Walking starts on the evening of surgery. This prevents blood clots and pneumonia.